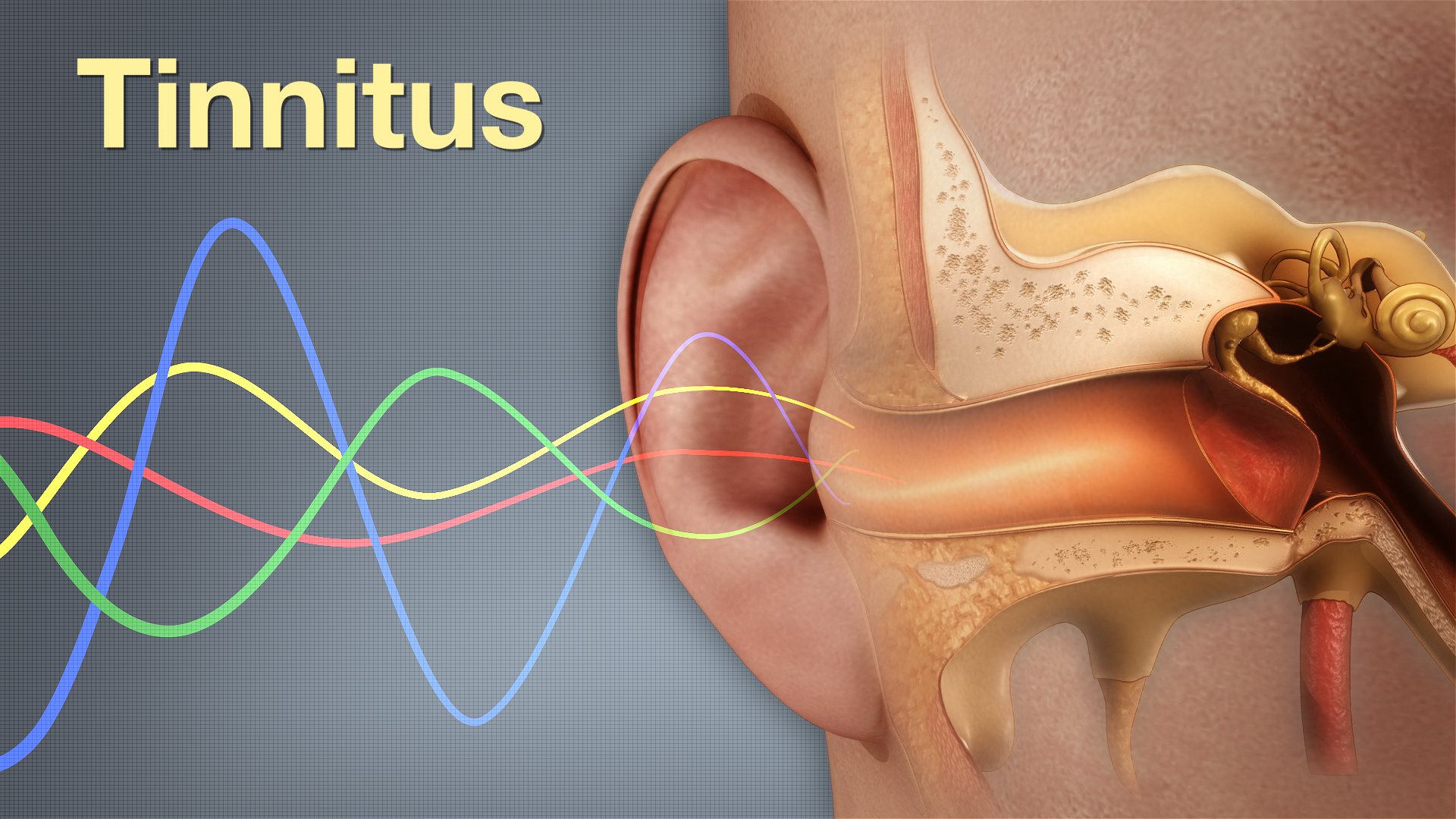
Most people describe it as a ringing or buzzing that never comes from any external source. Tinnitus feels internal, as if a noise is generated within the ear or brain. It varies—some hear high-pitched tones, others detect low-frequency hums or pulses. The sound can remain constant or shift throughout the day. It doesn’t follow external stimuli and can intensify in quiet rooms. Tinnitus often becomes noticeable during bedtime or periods of stress. Some experience it in one ear, others in both. Despite its presence, medical exams often reveal no visible damage. That contrast between hearing a sound and detecting nothing physically creates confusion and frustration.
One of the most common triggers is prolonged exposure to high-intensity noise environments
One of the most common triggers is prolonged exposure to high-intensity noise environments. Concerts, machinery, and headphones all contribute to cumulative auditory damage. Hair cells inside the cochlea vibrate in response to sound. Overstimulation damages or kills these cells, which don’t regenerate. When they malfunction, the brain receives distorted or absent input. That gap sometimes leads the brain to generate phantom signals interpreted as sound. Even short bursts of intense noise can cause damage. That’s why many tinnitus patients report onset after a single loud event. Musicians and industrial workers face higher risk due to frequent noise contact. Hearing protection is critical but often neglected.
Ear infections, wax buildup, and jaw disorders can also interfere with sound perception
Ear infections, wax buildup, and jaw disorders can also interfere with sound perception. When the outer or middle ear becomes inflamed or blocked, sound waves are disrupted. This disruption sometimes triggers abnormal neural signals interpreted as ringing. Temporomandibular joint (TMJ) issues also contribute. The joint lies close to ear structures, and misalignment affects nerves shared with auditory pathways. Some patients with tinnitus also report facial pain or jaw stiffness. Dental alignment, stress clenching, and posture habits may all influence symptom onset. In these cases, addressing the underlying mechanical problem may reduce the auditory disturbance. Tinnitus linked to temporary blockages usually resolves faster than cases from nerve damage.
Some medications list tinnitus as a possible side effect depending on dosage and patient sensitivity
Some medications list tinnitus as a possible side effect depending on dosage and patient sensitivity. Aspirin, certain antibiotics, antidepressants, and chemotherapy drugs have all been linked to auditory symptoms. These medications may affect neurotransmitters, blood flow, or inner ear chemistry. Tinnitus caused by drugs may emerge suddenly or develop gradually with repeated exposure. Patients taking high doses for extended periods often report increased symptoms. Stopping the drug sometimes reverses the effect, but not always. It’s important not to change medication without medical supervision. Alternative options may be available, but withdrawal must be managed properly. Patients should keep a log of dosage changes and auditory symptoms to aid diagnosis.
Neurological conditions involving nerve compression or abnormal activity may also play a role
Neurological conditions involving nerve compression or abnormal activity may also play a role. The auditory nerve carries sound signals from the ear to the brain. If compressed or irritated, it may send faulty signals. Multiple sclerosis and vestibular schwannomas (acoustic neuromas) are two examples. These conditions involve the nervous system and affect communication between sensory organs and the brain. Brainstem injuries or tumors may also produce tinnitus as a secondary symptom. Diagnosis often requires imaging like MRI to identify structural abnormalities. These cases are rare but important to consider when tinnitus is persistent, unilateral, or accompanied by hearing loss. Early intervention can prevent further complications.
Chronic stress and sleep disruption intensify tinnitus even without physical ear damage
Chronic stress and sleep disruption intensify tinnitus even without physical ear damage. Stress triggers heightened awareness of internal sensations, including background noise. It also affects hormone levels and increases muscle tension, especially in the neck and shoulders. These changes can aggravate the auditory system’s sensitivity. Poor sleep reduces the brain’s ability to filter irrelevant stimuli, making the sound more intrusive. Many patients report tinnitus worsening during emotionally intense periods. Cognitive factors like attention and anxiety amplify the perception further. Addressing stress isn’t a cure, but it lowers the intensity and emotional reaction to symptoms. Behavioral therapies often focus on reframing awareness and controlling physiological responses.
Standard hearing tests may appear normal even when symptoms are constant and disruptive
Standard hearing tests may appear normal even when symptoms are constant and disruptive. Audiograms measure how well someone hears external sounds across frequencies. But tinnitus isn’t an external sound, and tests may not detect internal distortions. Some patients with normal hearing report high levels of distress. This disconnect often leads to confusion or disbelief from others. Tinnitus can occur without measurable hearing loss. Advanced diagnostics like otoacoustic emissions or auditory brainstem response testing may reveal subtle changes. Still, many providers rely on self-reports and questionnaires to assess severity. Patient descriptions are critical in guiding treatment decisions. Silence in testing rooms doesn’t match the noise inside the patient’s mind.
Sound therapy introduces external tones that help mask or distract from internal ringing
Sound therapy introduces external tones that help mask or distract from internal ringing. White noise machines, nature sounds, or music playlists can reduce contrast between silence and tinnitus. The goal isn’t to eliminate the noise but to shift perception. By adding low-level background sound, the brain becomes less focused on the internal tone. Over time, it may reduce its significance. Some devices are worn like hearing aids and emit customized sounds. These are tailored to the frequency and loudness of the patient’s tinnitus. When used consistently, sound therapy promotes habituation—a process where the brain stops reacting emotionally to the noise.
Cognitive behavioral therapy helps reduce distress even when the auditory signal remains unchanged
Cognitive behavioral therapy helps reduce distress even when the auditory signal remains unchanged. CBT focuses on how thoughts and emotions influence perception. For tinnitus, the approach helps patients manage anxiety, depression, or sleep issues triggered by the sound. It doesn’t remove the noise but changes the relationship to it. Patients learn how to shift attention, challenge unhelpful beliefs, and adopt coping techniques. Group therapy, mindfulness, and relaxation strategies are often included. The therapy works best when combined with other treatments. Studies show it improves quality of life, especially for those whose tinnitus interferes with concentration or daily tasks.
Some patients find relief through dietary changes and reduction of stimulants like caffeine
Some patients find relief through dietary changes and reduction of stimulants like caffeine. Foods high in sodium or sugar may increase vascular tension and blood pressure, affecting ear circulation. Caffeine and alcohol can heighten nervous system activity, making the brain more alert to internal noise. Eliminating or reducing these substances sometimes leads to improvement. Others focus on increasing magnesium, zinc, or vitamin B12, which support nerve health. There’s no universal diet for tinnitus, but personal experimentation under guidance may uncover sensitivities. Keeping a symptom diary can identify patterns. Diet alone won’t cure tinnitus, but it may lessen severity in some individuals.
Devices like hearing aids or neuromodulation tools provide structured sound input to retrain the brain
Devices like hearing aids or neuromodulation tools provide structured sound input to retrain the brain. For patients with coexisting hearing loss, amplifying external sounds reduces internal focus. Neuromodulation tools use specific sound patterns to disrupt tinnitus-related brain activity. These devices often require programming by audiologists based on personal symptom profiles. While not effective for everyone, some experience partial or even lasting relief. The success depends on tinnitus type, duration, and individual brain response. These technologies represent a growing field that merges neuroscience with engineering. As understanding of brain plasticity improves, more targeted interventions may emerge over time.